Amazon Affiliate Disclosure: Geronutrition may earn from qualifying Amazon purchases and other affiliate links when an individual chooses to purchase through links on this page. This does not change editorial standards, recommendations, or the educational purpose of this guide.
A blood test for vitamin deficiency can reveal what the mirror, the bathroom scale, and a casual checkup often miss. After 60, fatigue may look like aging. Weak legs may be blamed on age. Brain fog may be dismissed as “normal.” Yet beneath those symptoms there may be low vitamin D, poor B12 absorption, insufficient protein status, chronic inflammation, dehydration, iron imbalance, impaired glucose control, or early malnutrition. At Geronutrition, the goal is to make aging nutrition measurable, practical, and connected to real-life function rather than guesswork.
This page explains how deficiency testing and longevity biomarker optimization work together. It is not about chasing perfect lab numbers or turning every meal into a medical project. It is about using the right measurements at the right time so an older adult can protect muscle, cognition, energy, bone strength, immunity, metabolic health, and independence.
A well-designed vitamin deficiency test does more than identify a low nutrient. It helps answer a sharper question: “Is this body receiving, absorbing, converting, transporting, and using the nutrients it needs to age well?”
Quick Picks: Jump to the Section You Need
Use this quick navigation to move directly to the most relevant part of the guide.
What a Blood Test for Vitamin Deficiency Is Really For
A blood test for vitamin deficiency is not just a pass-or-fail report card. It is a biological clue system. It can show whether an older adult has enough of certain nutrients in circulation, whether blood cells are being formed properly, whether inflammation is quietly rising, whether protein status is slipping, or whether metabolic stress is changing the body’s nutrient needs.
The mistake is thinking of deficiency testing as one isolated lab result. A low vitamin D result may matter, but it matters more when viewed beside calcium, kidney function, inflammation, fall risk, muscle weakness, and diet quality. A “normal” B12 result may still need context if an older adult has numbness, memory complaints, metformin use, acid-suppressing medication, or elevated methylmalonic acid. A low albumin result may not simply mean “eat more protein”; it may reflect inflammation, poor intake, liver disease, kidney loss, or a recovery state after illness.
The purpose of deficiency and biomarker optimization is to move from symptom guessing to pattern recognition.
What It Is For
A blood test for vitamin deficiency is mainly used to:
- Detect hidden nutrient gaps before they become functional decline
- Explain symptoms such as fatigue, weakness, low appetite, poor balance, cramps, numbness, brittle nails, slow recovery, low mood, or brain fog
- Evaluate whether diet, digestion, medication use, and absorption are meeting the needs of aging physiology
- Guide safe supplementation instead of random high-dose use
- Track whether a nutrition plan is working over time
- Connect nutrient status with longevity biomarkers such as inflammation, glucose control, muscle preservation, and protein reserves
The deepest value is not the test itself. The value is the decision it improves.
A lab result should change something: food choices, supplement dose, protein strategy, hydration pattern, medical follow-up, medication review, strength training, sleep timing, or chronic disease management. If a test does not help guide a better decision, it becomes expensive decoration.
Why Testing Matters More After 60
After 60, nutrient status becomes less predictable. Two people can eat the same breakfast and absorb, metabolize, and use it very differently. Aging changes stomach acid, muscle mass, appetite, kidney handling, inflammatory tone, medication exposure, gut motility, sunlight exposure, and recovery capacity. The body also becomes less forgiving. A small deficit that a 35-year-old could tolerate may become a fall, fracture, infection, depressive spiral, or hospital readmission risk in an older adult.
This is why geronutrition looks beyond calories. It asks whether the body is adequately supplied for resilience.
Who Needs a Vitamin Deficiency Test After 60?
Not every person needs every nutrient tested. More testing is not automatically better care. The right question is: who has enough risk, symptoms, medical history, or lifestyle change to justify a vitamin deficiency test?
A person over 60 may benefit from discussing testing with a clinician when there are symptoms, known risk factors, restricted diets, medication use, unexplained physical decline, or chronic disease patterns that make deficiencies more likely.
Higher-Risk Older Adults
The following groups deserve closer attention:
| Risk Pattern | Why Testing May Matter |
|---|---|
| Low appetite or unintentional weight loss | May reflect low protein intake, micronutrient gaps, inflammation, depression, dental issues, or illness |
| Limited sunlight exposure | Raises concern for vitamin D insufficiency, especially with low mobility or indoor living |
| Vegan or mostly plant-based diet | May increase risk of B12, iron, zinc, iodine, calcium, and protein gaps if not planned carefully |
| Metformin use | May be associated with lower B12 status over time |
| Acid-suppressing medications | May reduce absorption of B12, magnesium, iron, and other nutrients in some individuals |
| Frequent falls or muscle weakness | May connect with vitamin D, protein status, dehydration, anemia, inflammation, or sarcopenia |
| Memory changes or numbness | Can overlap with B12 deficiency, thyroid issues, glucose control, medication effects, or neurological disease |
| Chronic kidney disease | Changes vitamin D metabolism, mineral balance, protein strategy, and supplement safety |
| Diabetes or prediabetes | Increases the value of HbA1c, glucose patterns, B12 review, kidney markers, and inflammation assessment |
| Recent hospitalization | Often accelerates muscle loss, appetite loss, dehydration, and low protein reserves |
| Poor dentition or chewing difficulty | Can reduce intake of meat, vegetables, nuts, seeds, and high-protein foods |
| Long-term digestive symptoms | Raises suspicion for malabsorption, low intake, inflammatory bowel issues, celiac disease, or pancreatic insufficiency |
When Symptoms Should Trigger a Conversation
A vitamin deficiency test is especially relevant when the story does not fit a simple explanation.
For example, an older adult says, “I’m just tired because I’m old.” But the timeline matters. Did fatigue begin after a new medication? After a fall? After a period of low appetite? After moving indoors? After a diet change? After grief? After a respiratory infection? After months of poor sleep?
Symptoms become more meaningful when they are new, worsening, unexplained, or paired with physical decline.
Testing Is Not a Substitute for Clinical Judgment
A lab test can mislead when interpreted without context. Normal results can provide false reassurance. Abnormal results can create panic. The best approach is not “test everything.” It is targeted testing guided by age, symptoms, diet, medication history, physical function, and medical risk.
Benefits of Deficiency and Biomarker Optimization

Deficiency and biomarker optimization is not about living forever. It is about reducing avoidable decline. The aim is to protect function while there is still time to intervene.
The benefits are strongest when lab work is paired with food, supplements when appropriate, resistance training, hydration, sleep, medical review, and follow-up testing.
Benefit 1: Earlier Detection of Correctable Problems
Many deficiencies do not announce themselves clearly. B12 deficiency may look like fatigue, memory issues, numbness, mood change, or anemia. Vitamin D insufficiency may be invisible until bone or muscle risk becomes obvious. Iron deficiency may show up as breathlessness, weakness, restless legs, or poor exercise tolerance. Dehydration may look like confusion, dizziness, constipation, or low blood pressure.
Testing can bring the invisible into view.
Benefit 2: Better Supplement Decisions
Without labs, supplement use often becomes emotional. A person feels tired, buys a multivitamin, adds vitamin D, tries magnesium, adds collagen, then wonders which product is working. This scattered approach can be wasteful and sometimes unsafe.
A vitamin deficiency test helps separate “possibly useful” from “actually needed.” It also helps decide whether the issue is low intake, poor absorption, medication-related depletion, inflammation, kidney handling, or something that requires medical evaluation.
Benefit 3: Stronger Aging Nutrition Plans
A nutrition plan after 60 should not only ask, “What is healthy?” It should ask, “What does this person’s body need now?”
A frail older adult recovering from illness may need a different protein strategy than a metabolically stable active adult. A person with low B12 and high homocysteine may need a different plan than someone whose fatigue is driven by poor sleep and inflammation. A person with low albumin and weight loss needs a different conversation than someone with normal protein markers but low vitamin D.
Biomarkers make nutrition less generic.
Benefit 4: Reduced Risk of Overcorrection
High-dose supplementation without measurement can create problems. Fat-soluble vitamins, minerals, iron, calcium, and certain combinations should not be treated casually. Too much can be as relevant as too little.
Testing helps prevent the common pattern of taking multiple overlapping products without knowing total intake.
Benefit 5: Better Monitoring Over Time
One lab result is a photograph. Repeated testing, when appropriate, is a film.
The real question is not only “Is this marker low?” It is “Is the direction improving?” Albumin, vitamin D, HbA1c, CRP, kidney markers, blood count, ferritin, and muscle-related measures become more useful when tracked over time and interpreted alongside diet, strength, symptoms, and medication changes.
Nutrient Deficiencies in Older Adults: Why They Hide in Plain Sight
Nutrient deficiencies in older adults rarely appear as clean textbook cases. They often arrive disguised as ordinary aging.
An older adult may not say, “I think I have low B12.” They may say, “My feet feel strange.” They may not say, “I have a protein-energy problem.” They may say, “I don’t feel like eating meat anymore.” They may not say, “My hydration is poor.” They may say, “I get dizzy when I stand.”
This is why the Vitamin Deficiencies page is an important next step for readers who want deeper coverage of vitamin D, B12, magnesium, iron, protein, and dehydration patterns in aging.
Why Deficiencies Become Easier to Miss With Age
There are several reasons deficiency patterns get blurred after 60.
First, symptoms overlap. Fatigue may reflect anemia, B12 deficiency, low vitamin D, poor sleep, depression, thyroid disease, inflammation, heart disease, dehydration, low protein intake, or medication effects.
Second, diet history becomes unreliable. Many older adults eat “regular meals,” but those meals may be smaller, repetitive, low in protein, low in fiber, low in minerals, or missing nutrient-dense foods.
Third, absorption changes. A person may eat enough of a nutrient but fail to absorb or activate it properly.
Fourth, inflammation changes interpretation. Some blood markers shift during infection, chronic disease, obesity, autoimmune activity, or recovery after illness.
Fifth, the body compensates until it cannot. Muscle loss, bone loss, and cognitive strain may develop gradually before a dramatic symptom appears.
The Deficiencies That Matter Most in Aging Nutrition
The main deficiency concerns after 60 often include:
| Deficiency Concern | Why It Matters After 60 | Common Clues |
|---|---|---|
| Vitamin D | Bone strength, muscle function, immune support, fall risk context | Low sun exposure, weakness, bone discomfort, fracture risk |
| Vitamin B12 | Nerve function, red blood cell formation, cognition, methylation | Numbness, tingling, memory complaints, fatigue, anemia |
| Magnesium | Muscle relaxation, glucose metabolism, blood pressure support, sleep quality | Cramps, poor sleep, constipation, medication exposure |
| Iron | Oxygen transport, energy, exercise tolerance | Fatigue, breathlessness, pale skin, restless legs, anemia |
| Protein | Muscle preservation, immune function, wound healing, recovery | Weight loss, weakness, low grip strength, slow recovery |
| Hydration and electrolytes | Blood pressure, cognition, kidney function, bowel regularity | Dizziness, constipation, confusion, dark urine, low intake |
The word “deficiency” can sound small. In older adults, it can be the beginning of a cascade. Low appetite leads to low protein. Low protein accelerates muscle loss. Muscle loss increases fall risk. A fall reduces mobility. Reduced mobility lowers sunlight exposure. Low sunlight worsens vitamin D status. Reduced independence then reduces diet variety. One small gap becomes a system problem.
What Blood Tests Show Vitamin Deficiencies?
The question “what blood tests show vitamin deficiencies” deserves a careful answer because there is no single test that detects every deficiency with equal reliability.
Some nutrients are directly measured. Others are inferred through functional markers. Some markers are affected by inflammation, hydration, kidney function, liver function, recent meals, supplements, or acute illness. A smart testing strategy combines direct nutrient levels with supportive biomarkers.
Common Blood Tests for Vitamin and Nutrient Deficiency
| Nutrient or Concern | Common Blood Test or Marker | What It May Help Show | Important Context |
|---|---|---|---|
| Vitamin D | 25-hydroxyvitamin D | Vitamin D status | Interpretation varies by guideline, risk, symptoms, and clinical context |
| Vitamin B12 | Serum B12, methylmalonic acid, homocysteine | B12 availability and functional deficiency clues | Serum B12 alone can miss some cases; MMA may be more informative in certain situations |
| Folate | Serum folate or RBC folate | Folate status | Must be interpreted with B12 to avoid masking neurological risk |
| Iron | Ferritin, serum iron, transferrin saturation, TIBC, CBC | Iron stores and anemia patterns | Ferritin rises with inflammation, so context matters |
| Protein status | Albumin, prealbumin in select cases, total protein | Protein reserves, illness burden, malnutrition clues | Albumin is affected by inflammation and disease, not just protein intake |
| Anemia | CBC, hemoglobin, hematocrit, MCV, RDW | Red blood cell size and anemia pattern | Can suggest iron, B12, folate, chronic disease, or mixed causes |
| Magnesium | Serum magnesium, sometimes RBC magnesium | Magnesium status | Serum magnesium may not fully reflect tissue stores |
| Hydration and kidney handling | Sodium, potassium, chloride, BUN, creatinine, eGFR | Fluid balance and kidney function clues | Dehydration, medications, and kidney disease alter interpretation |
| Glucose metabolism | Fasting glucose, fasting insulin, HbA1c | Metabolic health and glycation pattern | HbA1c may be affected by anemia and red blood cell turnover |
| Inflammation | hs-CRP, ESR in some contexts | Inflammatory burden | Helps explain why nutrient markers may behave unexpectedly |
Direct Markers vs Functional Markers
A direct marker measures the nutrient or its storage form. A functional marker measures the biological consequence of not having enough of it.
For example, serum B12 measures circulating B12, but methylmalonic acid may rise when B12-dependent metabolism is impaired. Ferritin reflects iron stores, but ferritin can be elevated by inflammation, so transferrin saturation and CBC patterns may be needed. Albumin may fall in malnutrition, but it can also fall because of inflammation, liver disease, kidney disease, or acute illness.
This is why the best answer to “what blood tests show vitamin deficiencies” is not a single list. It is a pattern-based panel interpreted with the person’s symptoms and medical background.
A Practical Testing Map
| Health Question | Useful Lab Direction |
|---|---|
| “Why am I tired all the time?” | CBC, ferritin/iron studies, B12, folate, vitamin D, thyroid markers, HbA1c, kidney/liver markers |
| “Why am I weaker than last year?” | Vitamin D, protein markers, CBC, inflammation markers, HbA1c, kidney function, muscle assessment |
| “Could my memory issues be nutrition-related?” | B12, MMA if appropriate, folate, homocysteine, thyroid markers, HbA1c, vitamin D context |
| “Why do I feel dizzy or unsteady?” | CBC, electrolytes, hydration/kidney markers, glucose markers, medication review |
| “Am I absorbing nutrients well?” | B12/MMA, iron studies, vitamin D, albumin, CBC, digestive history, medication review |
| “Is my aging nutrition plan working?” | Repeat targeted markers after a reasonable interval, plus weight, strength, appetite, function, and symptoms |
Vitamin Deficiency Test Options: Clinic, Home and Advanced Panels

A vitamin deficiency test can be ordered through a physician, clinic, lab, wellness provider, or direct-to-consumer testing company depending on location, regulation, and medical need. Each route has advantages and limitations.
The most important issue is not convenience. It is interpretation.
A home test can be useful when it measures a clinically meaningful marker through a reputable lab and gives clear instructions. But a test result without clinical context can lead to overreaction, unnecessary supplements, or missed disease. A clinic-based test may be slower, but it can connect results with symptoms, medications, physical exam, diagnosis, and insurance coverage.
Comparison: Testing Routes
| Testing Route | Strengths | Limitations | Best Fit |
|---|---|---|---|
| Primary care or geriatric clinic | Medical interpretation, medication review, insurance pathway, follow-up care | May not test broad nutrition markers unless symptoms justify it | Older adults with symptoms, chronic disease, medication complexity |
| Specialist-directed testing | Deeper context for kidney, digestive, endocrine, hematology, or neurological concerns | More expensive, referral may be needed | Complex deficiency patterns or abnormal results |
| Direct lab order | Faster access, clear standard lab markers | May still require self-interpretation | Individuals who know exactly which markers they need and will review results clinically |
| Home collection kit | Convenient, useful for mobility-limited individuals | Sample quality, limited panels, interpretation issues | Basic screening when reputable lab processing and follow-up are available |
| Advanced longevity panel | Broad view of metabolism, inflammation, lipids, glucose, hormones, nutrient markers | Can be expensive and overwhelming | Data-driven individuals who want structured optimization with professional interpretation |
What Makes a Vitamin Deficiency Test Worth Paying For?
A good test should meet five standards:
- It measures a marker that can guide action
- It uses a reliable lab method
- It gives clear collection instructions
- It includes reference ranges and clinical caveats
- It encourages medical follow-up for abnormal or confusing results
A poor test creates more questions than answers. It may test too many low-value markers, use vague “optimal” ranges, imply diagnosis without context, or push supplements before the person understands the result.
Geronutrition serves all three intents, test intelligently, interpret carefully, supplement only when the result and context justify it.
Longevity Biomarkers That Turn Lab Work Into a Healthspan Map
Deficiency testing answers: “What might be missing?”
Longevity biomarker optimization asks: “How well is the body aging as a system?”
That distinction matters. An older adult may have adequate vitamin D and B12 but still show high inflammation, rising HbA1c, poor protein reserves, declining kidney function, low muscle mass, or worsening metabolic flexibility. Nutrient sufficiency is necessary, but it is not the whole map.
The Longevity Biomarkers page can expand this into specific blood markers such as vitamin D, homocysteine, CRP, albumin, HbA1c, muscle-related biomarkers, biological age testing, and longevity blood markers.
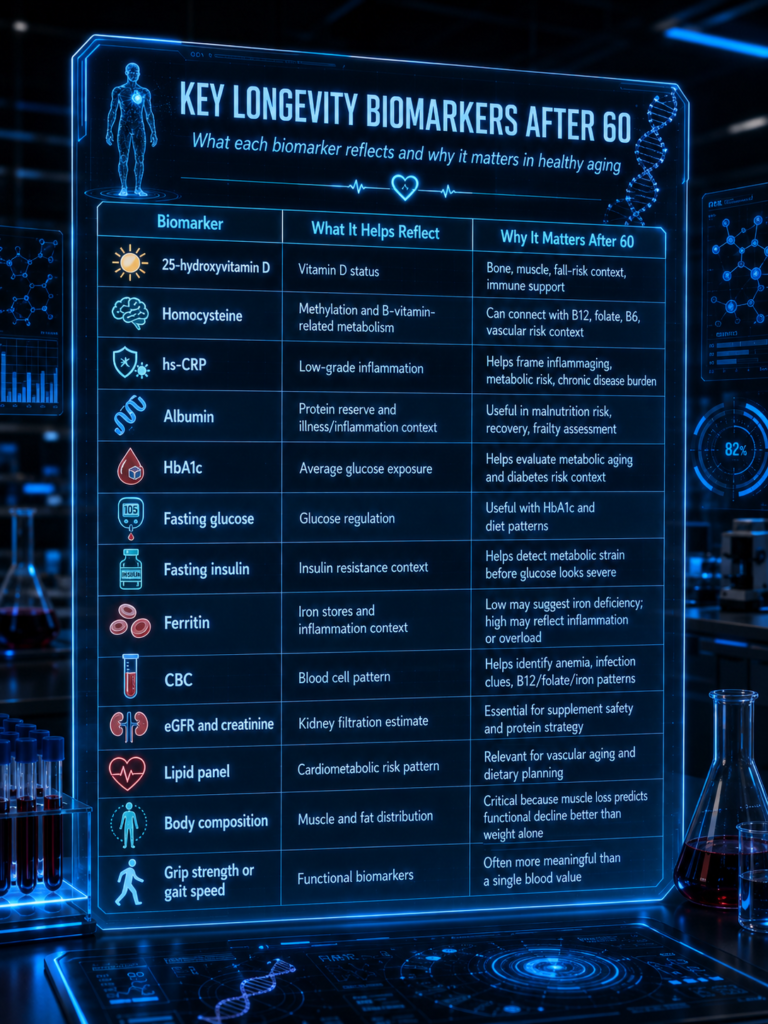
Key Longevity Biomarkers for Geronutrition
| Biomarker | What It Helps Reflect | Why It Matters After 60 |
|---|---|---|
| 25-hydroxyvitamin D | Vitamin D status | Bone, muscle, fall-risk context, immune support |
| Homocysteine | Methylation and B-vitamin-related metabolism | Can connect with B12, folate, B6, vascular risk context |
| hs-CRP | Low-grade inflammation | Helps frame inflammaging, metabolic risk, chronic disease burden |
| Albumin | Protein reserve and illness/inflammation context | Useful in malnutrition risk, recovery, frailty assessment |
| HbA1c | Average glucose exposure | Helps evaluate metabolic aging and diabetes risk context |
| Fasting glucose | Glucose regulation | Useful with HbA1c and diet patterns |
| Fasting insulin | Insulin resistance context | Helps detect metabolic strain before glucose looks severe |
| Ferritin | Iron stores and inflammation context | Low may suggest iron deficiency; high may reflect inflammation or overload |
| CBC | Blood cell pattern | Helps identify anemia, infection clues, B12/folate/iron patterns |
| eGFR and creatinine | Kidney filtration estimate | Essential for supplement safety and protein strategy |
| Lipid panel | Cardiometabolic risk pattern | Relevant for vascular aging and dietary planning |
| Body composition | Muscle and fat distribution | Critical because muscle loss predicts functional decline better than weight alone |
| Grip strength or gait speed | Functional biomarkers | Often more meaningful than a single blood value |
Biomarkers Are Not Trophies
A common mistake in longevity culture is treating biomarkers like achievements. Lower is not always better. Higher is not always better. Context decides.
For example, very low cholesterol may be concerning in a frail older adult with weight loss. Low HbA1c may look excellent but may not be ideal if driven by anemia, undernutrition, or frequent hypoglycemia. High ferritin may reflect iron overload, but it may also reflect inflammation. Low albumin may suggest poor protein status, but it may also reveal illness burden.
The body is not a spreadsheet. It is a living system. Biomarkers are signals, not commandments.
Vitamin Deficiency vs Aging Symptoms
One of the most valuable sections for search intent is the comparison between vitamin deficiency vs aging symptoms. Many older adults and caregivers struggle with this exact question: “Is this just age, or is something missing?”
The honest answer is that symptoms overlap. But timelines, severity, combinations, and lab patterns can help.
Comparison Table: Deficiency Clues vs Aging-Related Change
| Symptom | Could Be Nutrient-Related When… | Could Be Broader Aging or Disease When… |
|---|---|---|
| Fatigue | New or worsening, paired with low appetite, anemia, low B12, low vitamin D, low iron, dehydration | Persistent despite normal labs, linked with sleep apnea, heart disease, depression, thyroid disease, medication effects |
| Muscle weakness | Paired with low protein intake, low vitamin D, weight loss, low activity, inflammation | Progressive neurological disease, severe arthritis, heart/lung limitation, advanced frailty |
| Brain fog | Paired with B12 risk, dehydration, poor glucose control, low intake, medication changes | Dementia, sleep disorder, depression, infection, vascular disease |
| Numbness or tingling | Paired with B12 risk, diabetes, medication exposure | Neuropathy from diabetes, spine disease, nerve compression |
| Bone pain or fracture risk | Paired with low vitamin D, low calcium intake, low protein, limited sun | Osteoporosis, cancer, inflammatory disease, kidney disease |
| Dizziness | Paired with dehydration, low intake, anemia, electrolyte imbalance | Blood pressure medication, arrhythmia, vestibular problems, neurological disease |
| Poor wound healing | Paired with low protein, zinc risk, diabetes, low calories | Circulation problems, infection, vascular disease, steroid use |
| Low mood | Paired with B12, folate, vitamin D, low omega-3 intake, poor appetite | Depression, grief, isolation, sleep disruption, chronic pain |
How to Think Like a Clinician
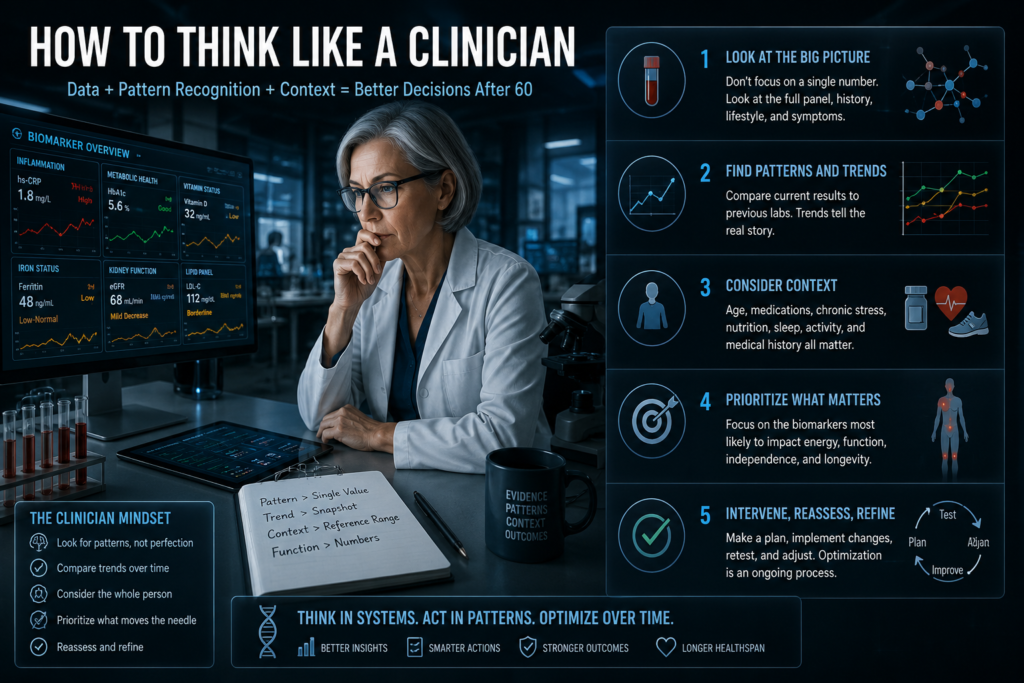
The sharper question is not “Which symptom belongs to which deficiency?” The sharper question is: “What changed?”
A gradual decline over ten years has a different meaning from a three-month collapse after poor appetite and inactivity. A person who eats well, walks daily, and has stable labs has a different risk pattern than someone who recently lost weight, stopped cooking, began metformin, and rarely goes outdoors.
Good deficiency evaluation begins with a story:
What changed?
When did it start?
What medications changed?
What foods disappeared?
What function was lost?
What lab markers moved?
What did the person stop doing?
This is how vitamin deficiency vs aging symptoms becomes more than a keyword. It becomes a clinical reasoning pathway.
The Geronutrition Biomarker Optimization Framework
Biomarker optimization after 60 should be practical. The goal is not to measure every possible marker. The goal is to create a loop: test, interpret, act, retest, refine.
A useful model is the S.T.A.R. framework.
S.T.A.R. Framework
| Step | Meaning | What It Looks Like |
|---|---|---|
| S | Screen | Identify symptoms, risk factors, diet gaps, medication issues, and basic labs |
| T | Translate | Interpret markers in context instead of reacting to one number |
| A | Act | Adjust food, hydration, protein, supplements, strength training, sleep, and medical care |
| R | Recheck | Retest targeted markers after a reasonable interval and compare with function |
Step 1: Screen
Screening begins before blood is drawn. A geronutrition screen should include appetite, weight change, diet variety, protein intake, hydration, chewing ability, swallowing difficulty, medications, supplement use, sunlight exposure, bowel patterns, falls, strength, sleep, and chronic disease history.
Basic lab work may include CBC, metabolic panel, vitamin D, B12, iron studies, HbA1c, lipids, kidney markers, liver markers, thyroid markers, and inflammation markers depending on the situation.
Step 2: Translate
Translation is where most mistakes happen.
A lab value should not be interpreted in isolation. For example:
Low vitamin D plus falls means something different from low vitamin D in a highly active person with no symptoms.
Low-normal B12 plus numbness and metformin use deserves more attention than the same value in someone without symptoms.
Low albumin after hospitalization may reflect acute inflammation and recovery, not simply poor food discipline.
High HbA1c plus low protein intake requires a careful food plan that improves glucose without worsening muscle loss.
Translation turns numbers into priorities.
Step 3: Act
Action should be specific. “Eat healthier” is too vague.
A better action plan might be:
Add 30 grams of protein at breakfast.
Use vitamin D supplementation only at a clinician-guided dose.
Replace tea-and-toast dinners with protein-rich soft meals.
Improve hydration before noon.
Review metformin and B12 status.
Use resistance bands three times weekly.
Recheck B12, vitamin D, CBC, and symptoms in a defined window.
Refer for evaluation if anemia, unexplained weight loss, kidney changes, or neurological symptoms appear.
The action should match the marker and the person.
Step 4: Recheck
Rechecking is not about obsession. It is about feedback.
If a person starts B12 supplementation, symptoms and markers should move in a meaningful direction. If vitamin D is corrected but weakness remains, the next step may involve protein, strength training, inflammation, neurological evaluation, or another cause. If HbA1c improves but weight and muscle fall, the nutrition strategy may be too restrictive.
Aging health improves when the plan is adjusted instead of defended.
Food, Supplements and Quick Recipes
Lab results should eventually reach the plate.
A blood test for vitamin deficiency may reveal what is missing, but food patterns determine whether the correction lasts. Supplements can be useful, especially for B12, vitamin D, iron, magnesium, protein, or other targeted needs. But supplements work best inside a nutrition system.
For meal-level support, connect this page with Quick Recipes so readers can move from lab insight to practical meals, soft-chew options, high-protein breakfasts, anti-inflammatory dinners, and caregiver-friendly food planning.
Food-First Does Not Mean Supplement-Never
Aging nutrition needs realism. Some deficiencies are difficult to correct with food alone, especially when absorption is impaired, sunlight exposure is limited, appetite is low, or medication changes nutrient handling. A person with B12 malabsorption may need supplementation even with a decent diet. A person with low vitamin D and minimal sun exposure may not correct it through food alone. A person with low protein intake may need protein powders or fortified meals when chewing, cooking, or appetite are barriers.
Food-first means the foundation is food. It does not mean ignoring biology.
Translating Common Results Into Nutrition Moves
| Lab Pattern | Nutrition Direction | Caution |
|---|---|---|
| Low vitamin D | Discuss D3 supplementation, fortified foods, safe sunlight exposure, fall-risk context | Avoid high-dose use without monitoring |
| Low B12 or high MMA | B12 supplementation route, medication review, animal or fortified foods if appropriate | Neurological symptoms need clinical attention |
| Low ferritin | Iron-rich foods, vitamin C pairing, evaluate bleeding risk | Do not take iron casually without diagnosis |
| Low albumin with weight loss | Protein distribution, calories, anti-inflammatory medical review | Albumin can reflect illness, not only diet |
| High HbA1c with muscle loss | Protein-preserving glucose strategy, fiber, meal timing, resistance training | Avoid overly restrictive diets |
| High hs-CRP | Anti-inflammatory diet pattern, weight, sleep, dental health, chronic disease review | CRP is nonspecific and needs context |
| Dehydration markers | Fluid rhythm, electrolytes when appropriate, medication review | Heart/kidney disease may require fluid limits |
The Plate Pattern After Testing
A practical geronutrition plate after lab testing often includes:
High-quality protein at each meal
Colorful plants for polyphenols and potassium
Calcium and vitamin D strategy for bone context
Fiber-rich carbohydrates adjusted to glucose tolerance
Healthy fats for energy and absorption
Hydration rhythm across the day
Texture modifications when chewing is difficult
Supplement support only when indicated
The goal is not perfection. The goal is repeatability.
Biomarkers for Chronic Disease Optimization
Deficiency testing becomes more powerful when linked with chronic disease patterns. Low B12 may matter more in diabetes because metformin exposure is common. Vitamin D, inflammation, glucose control, kidney function, and protein status matter in frailty and metabolic disease. Iron status matters when fatigue is blamed on aging but anemia is present. Albumin matters in recovery, wound healing, and malnutrition risk.
For a broader disease-focused nutrition strategy, this page should connect to Chronic Disease Optimization, where readers can explore condition-specific nutrition support for diabetes, osteoporosis, cognitive decline, frailty, heart health, kidney concerns, and inflammatory aging.
Why Chronic Disease Changes Nutrient Strategy
Chronic disease changes the meaning of nutrition.
A person with kidney disease may need careful protein, potassium, phosphorus, magnesium, vitamin D, and supplement review. A person with diabetes may need glucose control without sacrificing muscle. A person with osteoporosis needs bone nutrition, but also protein, strength, balance, and fall-risk reduction. A person with cognitive decline may need B12, hydration, omega-3 intake, protein, and stable glucose patterns reviewed alongside medical care.
The older adult body does not separate “vitamins” from “disease.” They interact.
Deficiency and Chronic Disease Map
| Condition Pattern | Biomarkers Worth Discussing | Nutrition Angle |
|---|---|---|
| Diabetes or prediabetes | HbA1c, fasting glucose, fasting insulin, B12, kidney markers, lipids | Glucose control while preserving muscle and B12 status |
| Osteoporosis or fracture risk | Vitamin D, calcium context, kidney markers, protein status | Bone support plus muscle and fall prevention |
| Cognitive symptoms | B12, MMA if appropriate, folate, homocysteine, HbA1c, thyroid, hydration markers | Nutrient sufficiency plus vascular and metabolic support |
| Frailty or sarcopenia | Albumin context, vitamin D, inflammation, CBC, body composition, grip strength | Protein, calories, resistance training, inflammation review |
| Chronic inflammation | hs-CRP, ferritin context, glucose markers, lipids | Anti-inflammatory eating pattern and root-cause assessment |
| Heart health | Lipids, HbA1c, hs-CRP, kidney markers, homocysteine context | Fiber, protein quality, sodium strategy, cardiometabolic nutrition |
| Kidney disease | eGFR, creatinine, electrolytes, albumin, vitamin D-related markers | Supplement safety and individualized protein/mineral guidance |
How to Use Supplement Reviews Without Chasing Pills
Supplement decisions after 60 should be evidence-informed, lab-aware, and safety-first. The market makes every capsule sound essential, but older adults need fewer random products and more targeted reasoning.
Readers can use Supplement Reviews to compare forms, doses, safety considerations, ingredient quality, and use cases after they understand what their biomarkers suggest.
The Supplement Decision Ladder
Before starting a supplement, ask:
- Is there a documented deficiency, risk factor, or clinical reason?
- Can food realistically correct the gap?
- Is absorption a problem?
- Does the person take medications that interact with the supplement?
- Is kidney or liver function relevant?
- Is the dose appropriate for age and lab status?
- When will the marker or symptom be reassessed?
A supplement without a recheck plan is often just hope in capsule form.
Supplement Categories That Commonly Connect With Testing
| Supplement Category | When It May Be Relevant | Why Testing Helps |
|---|---|---|
| Vitamin D | Low levels, low sun exposure, older age risk, bone health context | Helps avoid underdosing or excessive dosing |
| Vitamin B12 | Low B12, high MMA, metformin use, vegan diet, neurological symptoms | Helps choose oral, sublingual, or injection discussion |
| Iron | Confirmed iron deficiency or anemia pattern | Prevents unsafe iron use when not needed |
| Magnesium | Low intake, medication-related risk, cramps, glucose context | Helps assess safety, especially with kidney concerns |
| Protein powder | Low intake, frailty, poor appetite, sarcopenia risk | Helps support measurable muscle and recovery goals |
| Omega-3 | Low fish intake, inflammatory or cardiometabolic context | Best used as part of a broader plan |
| Multivitamin | Restricted diet or multiple mild gaps | Should not replace targeted correction |
Avoid the “Stacking” Problem
Many older adults take several products that overlap. A multivitamin, bone formula, immunity formula, sleep supplement, electrolyte powder, and protein shake may duplicate vitamin D, magnesium, zinc, calcium, B6, or other ingredients.
Stacking becomes risky when no one calculates total intake.
A safer approach is to list every supplement, include doses, review medications, check relevant labs, and remove what does not have a clear job.
Upcoming Trends and Latest Tech
The future of deficiency and biomarker optimization is moving toward earlier detection, easier collection, and more personalized interpretation. But the technology must be handled with caution. More data does not automatically mean better health.
Trend 1: At-Home Lab Collection With Professional Interpretation
Home vitamin deficiency test kits are becoming more common. The best versions combine convenient collection with certified lab processing, clear instructions, and clinician-guided interpretation. The weaker versions give isolated numbers with lifestyle advice that may not fit an older adult’s medical reality.
For seniors, the future is likely not “test yourself and figure it out.” It is home collection plus professional review.
Trend 2: Nutrient Testing Connected to Medication Risk
Medication-nutrient interaction screening will become more important. Metformin and B12, acid suppression and mineral/B12 concerns, diuretics and electrolytes, statins and muscle symptoms, and polypharmacy-related appetite changes are already practical issues. Future geronutrition platforms may connect medication lists with deficiency risk scoring.
Trend 3: Continuous Glucose Monitoring for Precision Meals
Continuous glucose monitors are already used in diabetes care and are expanding into metabolic wellness. For older adults, the most useful application may be identifying meal patterns that spike glucose while still preserving protein, calories, and muscle.
The caution is important: a glucose curve is not the full story of nutrition. A meal that produces a lower glucose response is not automatically better if it is too low in protein, fiber, micronutrients, or calories.
Trend 4: Biological Age Testing With Better Interpretation
Biological age testing is gaining attention, especially epigenetic clocks and multi-marker longevity panels. These tools may become more useful as interpretation improves. For now, they should not distract from boring but powerful fundamentals: muscle mass, strength, blood pressure, glucose control, inflammation, sleep, nutrition adequacy, kidney function, and physical activity.
The future may measure aging more precisely, but the core interventions will still happen in daily life.
Trend 5: Digital Biomarkers From Wearables
Wearables can already track sleep, resting heart rate, activity, heart rate variability, oxygen saturation trends, and movement patterns. For aging adults, these may become early warning signals for reduced resilience, infection, declining mobility, poor recovery, or frailty risk.
The strongest future model will combine blood biomarkers with functional biomarkers: labs plus grip strength, gait speed, sleep, steps, recovery, and real food intake.
Trend 6: Personalized Protein and Muscle Monitoring
As sarcopenia becomes a larger public health issue, muscle biomarkers will become more practical. Expect more attention to body composition scans, grip strength, gait speed, creatinine-to-cystatin C patterns, amino acid adequacy, protein distribution, and resistance-training response.
For geronutrition, muscle is not cosmetic. It is metabolic infrastructure.
Trend Table: What Is Emerging and What Still Needs Caution
| Trend | Promise | Caution |
|---|---|---|
| At-home deficiency testing | Convenience for mobility-limited adults | Needs proper sample handling and interpretation |
| Advanced nutrient panels | Broader view of deficiencies | Can overwhelm and overdiagnose |
| CGM-guided nutrition | Personalized glucose response | May ignore protein, calories, and overall diet quality |
| Biological age testing | Motivating healthspan snapshot | Not always clinically actionable |
| Wearable biomarkers | Continuous function and recovery data | Accuracy varies by device and user |
| Medication-nutrient risk scoring | More targeted deficiency prevention | Requires accurate medication history |
| Muscle-focused biomarker tools | Better sarcopenia detection | Needs functional testing, not just lab work |
Common Mistakes in Deficiency Testing
Deficiency testing can be powerful, but only when used well. These are the mistakes that create confusion.
Mistake 1: Testing Without a Question
A test should answer a question. “Am I low in anything?” is too broad. “Could low B12 or iron explain my fatigue and numbness?” is better. “Is my vitamin D status relevant to falls and low sun exposure?” is better. “Is my protein status contributing to slow recovery?” is better.
A sharp question leads to a better panel.
Mistake 2: Treating Reference Ranges as Personal Targets
Reference ranges are not always the same as optimal targets, and “optimal” ranges are not always agreed upon. Older adults also vary widely by medical history, kidney function, inflammation, medications, and frailty.
The number must be interpreted inside the person.
Mistake 3: Ignoring Symptoms Because the Test Is “Normal”
Normal does not always mean resolved. A person may have symptoms from a marker not tested, a functional deficiency, medication effects, sleep disorder, neurological disease, inflammation, or another medical issue.
If symptoms persist, the story is not over.
Mistake 4: Taking Iron Without Confirmation
Iron is not a casual supplement. Low iron needs explanation, especially in older adults, because blood loss, digestive disease, inflammation, or other medical problems may be involved. Taking iron without proper evaluation can delay the real diagnosis or cause harm.
Mistake 5: Correcting Vitamin D but Ignoring Muscle
Vitamin D matters, but fall prevention is not a vitamin D project alone. Muscle strength, balance, protein intake, vision, footwear, medications, home safety, hydration, and neurological function all matter.
A lab correction is not the same as functional recovery.
Mistake 6: Testing Too Soon After Starting a Supplement
Some markers need time to respond. Retesting too early may create unnecessary changes. The interval depends on the marker, severity, dose, medical condition, and clinician plan.
Mistake 7: Forgetting the Food Pattern
A supplement can correct a lab value while the diet remains fragile. If an older adult still eats too little protein, too few plants, too little fluid, and too few mineral-rich foods, the deeper risk remains.
Editorial Insights
A blood test for vitamin deficiency is one of the most practical entry points into modern geronutrition because it connects symptoms with measurable biology. But the best use of testing is not to create anxiety around every lab value. It is to identify leverage.
After 60, the body becomes more sensitive to small nutritional gaps. Low B12 can disturb nerves and cognition. Low vitamin D can sit quietly beside weak muscles and fracture risk. Low protein intake can accelerate sarcopenia before weight loss looks dramatic. Dehydration can mimic confusion. Inflammation can distort markers. Poor glucose control can age blood vessels, muscle, and brain tissue together.
The future of aging nutrition will not be built on one miracle supplement. It will be built on pattern recognition: nutrient markers, inflammation, metabolism, muscle, medication exposure, diet quality, and function moving together.
The smartest approach is simple but not simplistic:
Test what matters.
Interpret the pattern.
Correct what is correctable.
Retest with purpose.
Protect muscle, cognition, bone, metabolism, and independence.
For readers building a complete healthy aging plan, return to Geronutrition and connect deficiency testing with food strategy, supplement intelligence, chronic disease support, and longevity nutrition.
FAQs
What is the best blood test for vitamin deficiency after 60?
The best blood test for vitamin deficiency after 60 depends on the symptoms and risk factors. A practical starting point often includes CBC, vitamin D, vitamin B12, folate, iron studies, metabolic panel, kidney function, liver function, HbA1c, and sometimes magnesium, homocysteine, methylmalonic acid, thyroid markers, or inflammation markers. No single blood test detects every deficiency accurately.
For example, vitamin D is usually assessed with 25-hydroxyvitamin D. B12 may require serum B12 plus methylmalonic acid or homocysteine when symptoms or risk factors are present. Iron status usually needs ferritin, transferrin saturation, and CBC context rather than serum iron alone. Older adults should discuss testing with a clinician because medications, kidney function, inflammation, anemia, and chronic disease can change interpretation.
How often should older adults get a vitamin deficiency test?
Older adults do not need constant vitamin deficiency testing unless there is a medical reason. Testing may be reasonable when symptoms appear, diet changes, weight loss occurs, new medications are started, chronic disease worsens, falls increase, or a previous deficiency is being monitored.
A person with corrected vitamin D or B12 deficiency may need follow-up testing after an appropriate interval. A person with stable health, varied diet, no symptoms, and no major risk factors may not need frequent nutrient panels. The best schedule is individualized because over-testing can create confusion and unnecessary supplementation.
Can a vitamin deficiency test explain fatigue in seniors?
A vitamin deficiency test can help explain fatigue in seniors when fatigue is related to anemia, low B12, low iron, low vitamin D, poor protein status, dehydration, glucose problems, or other measurable issues. However, fatigue is broad. It can also come from sleep apnea, depression, infection, heart disease, thyroid disorders, chronic pain, medication effects, kidney disease, or inactivity.
The strongest approach is to combine lab testing with a symptom timeline. When did fatigue begin? Did appetite change? Is there weight loss? Are there new medications? Is sleep poor? Are there signs of anemia, numbness, weakness, dizziness, or low mood? Testing becomes more useful when attached to a clear clinical story.
What nutrient deficiencies in older adults are most commonly missed?
Nutrient deficiencies in older adults that are commonly missed include vitamin D, vitamin B12, protein insufficiency, iron deficiency, magnesium insufficiency, dehydration, and sometimes folate or zinc depending on diet and medical history. The reason they are missed is that symptoms often look ordinary: fatigue, weakness, low appetite, poor balance, brain fog, cramps, constipation, or slow recovery.
Protein insufficiency is especially under-recognized because many older adults maintain body weight while losing muscle. Dehydration is also missed because thirst sensation may decline with age. B12 deficiency can be missed when symptoms are neurological rather than purely blood-related. Testing helps, but diet history and function matter just as much.
Is a home vitamin deficiency test accurate enough for seniors?
A home vitamin deficiency test can be useful if it uses reliable collection methods, certified lab processing, clear instructions, and appropriate follow-up. It is less useful when it gives isolated numbers without medical context. For seniors with chronic disease, multiple medications, kidney concerns, neurological symptoms, anemia, weight loss, or frailty, clinician-guided testing is usually safer.
Home testing may work well for basic screening or monitoring when the person understands what the test can and cannot show. Any abnormal, severe, confusing, or symptom-linked result should be reviewed with a qualified healthcare professional.
People Also Ask
What blood tests show vitamin deficiencies?
Blood tests that may show vitamin deficiencies include 25-hydroxyvitamin D for vitamin D, serum B12 with methylmalonic acid or homocysteine for B12 context, folate testing, iron studies for iron deficiency, CBC for anemia patterns, metabolic panel for kidney and electrolyte context, and albumin or total protein for protein and illness-related clues.
Some tests show direct levels. Others show functional consequences. For example, a high methylmalonic acid level may suggest B12-related metabolic stress. A CBC may show large red blood cells in some B12 or folate problems, or small red blood cells in some iron deficiency patterns. Interpretation should always include symptoms, diet, medications, inflammation, and medical history.
Can vitamin deficiency symptoms look like normal aging?
Yes, vitamin deficiency symptoms can look like normal aging. Fatigue, weakness, poor balance, memory complaints, low mood, numbness, cramps, dizziness, and slow recovery are often blamed on age. Sometimes aging is part of the picture, but sometimes a correctable deficiency is contributing.
The key is to look for changes. New fatigue, recent weight loss, reduced appetite, numbness, falls, low sunlight exposure, restricted diet, medication changes, or worsening mobility should not be dismissed. A targeted vitamin deficiency test may help separate normal aging from treatable nutritional gaps.
What is the difference between a vitamin deficiency test and a longevity biomarker test?
A vitamin deficiency test looks for specific nutrient gaps such as vitamin D, B12, folate, iron, or related markers. A longevity biomarker test looks more broadly at aging biology, including inflammation, glucose control, lipid patterns, protein status, kidney function, body composition, and sometimes biological age measures.
The two approaches overlap. For example, low B12 can affect homocysteine, low vitamin D can connect with muscle and bone risk, and low protein status can affect frailty markers. Deficiency testing asks what may be missing. Longevity biomarker testing asks how well the body is functioning as an aging system.
Are vitamin deficiency blood tests better than symptom checklists?
Vitamin deficiency blood tests are more objective than symptom checklists, but they are not perfect. Symptom checklists are useful for deciding what to test. Blood tests are useful for confirming, ruling out, or refining suspicion. The best approach uses both.
A person with fatigue, numbness, and metformin use may need B12-related testing. A person with falls and low sun exposure may need vitamin D context. A person with weight loss and weakness may need protein, inflammation, blood count, and metabolic review. Symptoms guide the search; labs sharpen the answer.
Can supplements fix abnormal biomarkers after 60?
Supplements can improve abnormal biomarkers when the marker reflects a correctable nutrient gap and the supplement is appropriate. Vitamin D, B12, iron, magnesium, protein, and other nutrients may help when properly matched to deficiency, risk, and medical context.
However, supplements cannot fix every abnormal biomarker. High CRP may require inflammation source evaluation. High HbA1c may need meal pattern changes, activity, sleep, medication review, and weight or muscle strategy. Low albumin may reflect illness, inflammation, or organ disease. Supplements should be part of a plan, not a substitute for diagnosis or lifestyle structure.